
Integrating health into urban planning towards sustainability in Asian cities: Workshop summary
Keywords
Developing countries · Health impact assessment tools · Participatory · Policy integration · Urban planning
Highlights
- The workshop trained 38 participants from nine Asian countries.
- Guidelines and good practices for integrating health in urban planning were shared.
- Intersectoral and community engagement are essential for program sustainability.
- Low data quality may complicate the use of assessment tools in developing countries.
1. Introduction
Urban planning is a general term that can encompass several different fields in a city, depending on the contemporary needs of the respective country (Levy, 2017). From housing, town planning, landscaping, design, transport infrastructure, waste management, to biodiversity and forestry, agriculture, and disaster response, urban planning can have important implications across a country’s economy, sustainability, resilience and human wellbeing (de Leeuw & Simos, 2017; Levy, 2017). To that end, indicators have also been developed to measure a city’s liveability such as safety, walkability, availability of public spaces, etc., which are closely related to many planning parameters (Badland et al., 2014; Pineo et al., 2018). For the present paper, we refer to urban planning as the planning of physically built environments in cities.
Following rapid urbanization worldwide, sustainable development has been a pivotal global change concept that is incorporated in the foundations of all urban governing sectors, including urban planning (Wheeler & Beatley, 2014). On the other hand, sustainable development and population health are mutually reinforcing elements in urban systems (Webb et al., 2017). Sustainable development promotes an environment that induces healthy behaviour, reduces population exposure to harmful environmental health determinants that are fundamental to disease prevention, and ensures a healthy population, which is the central driving force to the sustainable development (Acharya, Lin, & Dhingra, 2018).
Urban planning in relation to sustainability and public health has been studied extensively in the past two decades (Mueller et al., 2017). A large amount of evidence points out that urban design such as high density and mixed land use, together with transit oriented development (TOD) could create an enabling environment for reducing traffic emissions and increasing.
population physical activity through alternative transport (Stevenson et al., 2016). Early incorporation of health in urban planning, especially during the development phase as in the Asian low and middle income countries (LMICs), could avoid the need for costly transformative urban restructuring for health mitigation and adaptation later (Chan & Li, 2016). To facilitate policy integration from multiple government sectors in a holistic perspective, approaches such as co-benefits and Health in All Policies (HiAP) have also been introduced (refer to Box 1).
Box 1. Definition of terms
|
This paper presents a workshop summary of “Integrating Health into Urban Planning towards Sustainable Development Goals in Developing Countries” on the presentations conducted to enhance awareness and knowledge of integrated assessment tools that can facilitate the integration of health in urban planning, from policymaking to implementation.In public policy making, sustainability strategies are usually prioritized and carried out based on their socio-economic values and returns (Macmillan et al., 2014). In the Asian cities of LMICs, poor health information caused by lack of system infrastructure and training has rendered limited quantifiable health evidence that can be used to inform policies from the public health perspective (Walsham, 2019). Integrated health assessment tools are useful to facilitate measurements of health progress and subsequently, the impacts of potential development projects. This can be undertaken qualitatively or quantitatively and can enhance negotiations, and inform policy decision making (WHO, 2014). Established integrated health assessment tools that have combined reliable data such as standard emission factors and disease relative risks sourced from robust systematic reviews of studies in developed countries can bridge evidence gaps in developing countries, and facilitate the quantification of health impacts to be fed into the policymaking process. By identifying policies that may help or hinder their objectives, trade-offs can be minimized to achieve the most beneficial results from the limited resources in developing countries (Hutton et al., 2018).
2. Methodology
A workshop on “Health in Urban Planning” was held at the University Selangor, Shah Alam Campus, Malaysia from 3-5 April 2019. There were 25 applicants from 17 cities and five local Malaysians who were screened and selected based on their background to join the workshop under the sponsorship of Asia Pacific Network for Global Change CAPaBLE Program (Box 2). The international participants were from Phnom Penh (Cambodia); Xiamen, and Guangzhou (China); Bathinda, and Gurgaon (India); Padang, Bangka, Andalas, Bandung (Indonesia); Vientiane (Lao PDR); Davao, Quezon City, Batangas (Philippines); Bangkok and Ayutthaya (Thailand); Hanoi and Ho Chi Minh (Viet Nam) (Figure 1). Other local participants included two staff from the Ministry of Health Malaysia, a representative from Kuala Lumpur City Hall, and five academics from University Selangor. Besides, 10 local and international experts on urban planning, environmental health, and sustainability from Kuala Lumpur, Jakarta, Bangkok, Sydney, Melbourne, Christchurch, Dunedin, Tokyo, and Cambridge were invited as speakers (Table 1). The speakers were invited based on their expertise and experiences in urban planning and health (No.1-7), and the application and development of tools for integrated assessment and decision making (No. 8-11) (Figure 2).
|
Box 2.
|
The workshop participants consisted of academics, policymakers, practitioners and a media reporter to have representatives of different roles in the workshop. The backgrounds of the participants included environmental science, public health, urban governance, climate change, urban geography, hydrology, urban ecology, disaster rehabilitation, health systems, and economy. Such diversity complemented the need for interdisciplinary and intersectoral communications in tackling planning in the complex urban systems in developing countries.


|
Theme |
Presenter/affiliation |
Presentation |
|
|
|
Empirical knowledge and good practices |
Jamal Hisham Hashim Universiti Selangor, Malaysia |
Urban Health Issues in Malaysia |
|
2.
|
Hj Ihsan Zainal Mokhtar Malaysian Institute of Planners, Malaysia |
Integrating Health Concept into Urban Planning in Malaysia | |
|
3.
|
Budi Haryanto Research Center for Climate Change, University of Indonesia, Indonesia |
Climate Change and Air Pollution: Health Impacts and Alternative Control Strategy | |
|
4.
|
Piyawat Katewongsa Institute for Population and Social Research, Mahidol University, Thailand |
The situation of physical activity promotion and built environment in Thailand | |
|
5.
|
Anna Stevenson Canterbury District Health Board, Christchurch, New Zealand |
Determinants Led Planning in Practice | |
|
6.
|
Alice Covatta The Architecture and Urban Design at co+labo, Keio University, Tokyo, Japan / The Centre for Urban Design and Mental Health |
Density and Intimacy in Public Space: a case study of Jimbocho, Tokyo’s book town | |
|
7.
|
Susan Thompson City Futures Research Centre, University of New South Wales, Australia |
Healthy Built Environments in Action! Experiences in policy and practice implementation | |
|
8.
|
Assessment tools |
Jamal Hisham Hashim Universiti Selangor, Malaysia |
Health Impact Assessment as a Planning and Decision-Making Tool |
|
9.
|
Jason Thompson Melbourne School of Design, University of Melbourne, Australia |
The Development of A Low-Carbon Living Co-Benefits Calculator | |
|
10.
|
James Woodcock MRC Epidemiology Unit, University of Cambridge, United Kingdom |
Modelling Transport Related Health Effects in Low and Middle Income Countries (LMICs) | |
|
11.
|
Alexandra Macmillan Department of Preventive and Social Medicine, University of Otago, New Zealand |
Using Systems Thinking and Modelling to Support Decision-Making for Healthy Sustainable Cities |
Table 1. List of invited presentations.
3. Results and discussion
3.1 Urban sustainability, health and urban planning good practices
Climate change and air pollution are the most common topics that are being emphasized in many urban sustainability discussions as the emissions of greenhouse gas often come together with air pollutants such as particulate matter (PM), nitrogen oxides (NOx), carbon monoxide (CO), and hydrocarbons (HCs) emissions from sources such as power plants and vehicle tailpipes (Driscoll, Stettler, Molden, Oxley, & ApSimon, 2018; Winkler et al., 2018). Air pollution is known to have caused a high burden of diseases, especially from cardiovascular and respiratory diseases. Based on the IPCC report, urban areas accounted for 67-76% of energy use and three-quarters of carbon emissions globally (IPCC, 2014). As urban growth accelerates, especially in Asian megacities, urban areas become the focus for mitigating carbon and air pollutant emissions through urban infrastructures that shape the energy use patterns in human and transport activities (Creutzig et al., 2015).
Non-communicable diseases (NCDs) accounted for 71% (41 million people) of global mortality in 2016, mainly from cardiovascular diseases, chronic respiratory diseases, cancers and diabetes (Bennett et al., 2018). In particular, a large proportion of preventable premature mortality from NCDs (40%) was contributed by the low and middle income countries, including Southeast Asia (Martinez et al., 2020). Although the risk factors for NCDs are well established, a review of evidence identifying the targeted reduction of NCD risk factors to impact on several NCDs simultaneously found that the improvement of physical inactivity, diet and air pollution have the strongest protective effects across cardiovascular diseases, cancer, diabetes, and dementia (Peters et al., 2019). These risk factors could be addressed in effective public policies and health interventions to reduce the number of preventable premature mortality (Martinez et al., 2020).
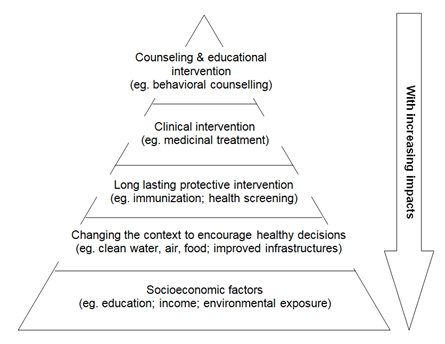
Urban planning can serve as an effective intervention to reduce the risk factors of NCDs by creating contextual defaults that empower behaviours to benefit both health and the environment (Frieden, 2010). Placed in the second tier of the Health Impact Pyramid (Figure 3), urban planning can affect human health and well being at the population level through the provisions of a clean environment and infrastructure. Table 2. shows the extraction of contents on good practices from the workshop presentations. These good practices and approaches could be useful guiding principles in building healthy cities, by integrating various health determinants including physical and mental health in urban planning related policies, funding allocations, implementation strategies, and community empowerment programs.
| Theme (country) | Key points and good practices | |
| 1. | Determinants led planning (Christchurch, New Zealand) |
|
| 2. | Integrating health in urban planning (Malaysia) |
|
| 3. | Experiences in policy and practice implementations (Australia) |
|
| 4. | Built environment and physical activity (Bangkok, Thailand) |
|
| 5. | Mental health: Density and intimacy in public space (Tokyo, Japan) |
|
Table 2. Key points and examples of good practice from workshop presentations.
3.2 Tools
3.2.1 Health impact assessment (HIA)
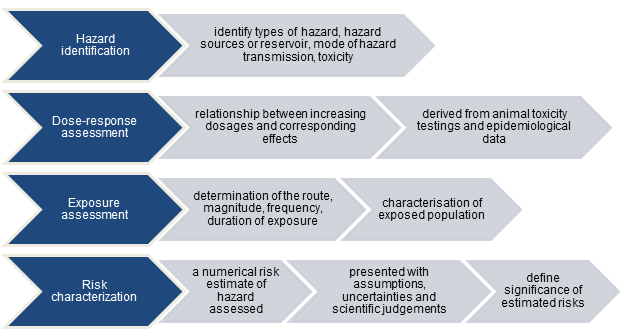
Health impact assessment (HIA) is a combination of procedures, methods and tools that are used to estimate the potential impacts (physical, chemical, biological, social) on a specified human population system under a specific set of conditions (a policy, program or a project) within a certain timeframe (enHealth, 2001). It is useful to inform and influence decision making by weighing in the evidence of health impacts from alternative development plans (Lock, 2000). In Malaysia, HIA is mandatory for many detailed Environmental Impact Assessment (EIA) project under prescribed activities. Figure 4 shows the steps involved in the HIA guidance document of Malaysia (Department of Environment Malaysia, 2012). An example of HIA application was given on the case of Kim Kim River in Pasir Gudang, Johor, where toxic chemical dumping (hazard identification) caused elevated levels of methane, benzene, and acrylonitrile (dose-response assessment) in the river, and hospitalization of poisoned victims among school children (exposure assessment) (The Straits Times, 2019).
3.2.2 Low carbon living co-benefits calculator
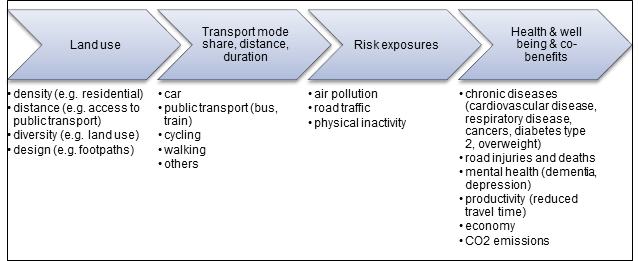
The model was built on the deterministic model of compact cities and health model connecting land use, transport mode, risk exposures and health outcomes (Stevenson et al., 2016) (Figure 5). Using 1.2 million of household land parcels with specific land use variables from the Australian Urban Research Infrastructure Network (AURIN), counts of features such as household density, public transport stops, number of intersections were captured. These variables were then used to develop a set of regression equations with the data of socio-demography, economy, productivity, and health from the Department of Health and Human Services Victorian Population Health Survey to estimate the co-benefits (Stevenson & Thompson, 2019). On the website interface of the calculator (https://thud.msd.unimelb.edu.au/), data can be input directly to generate performance outputs such as BMI and life satisfaction based on land use clusters. Although this tool applies in the Australian context, it presents a useful example of the methods and data needed to calculate co-benefits of specific land use planning in other cities.
3.2.3 Integrated transport and health impact model
Compared to the low carbon living co-benefits calculator, the model emphasizes on estimates of health impacts from different transport scenarios through distinctive models for air pollution, injuries and physical activity (Woodcock, Givoni, & Morgan, 2013). The primary data are from travel surveys, physical activity surveys (for non-travel physical activity), and police records of injury. In order to be a globally applicable tool, prototype models are being tested in countries such as India, Latin America and Africa with different traffic mix and background air pollution, injury and physical activity levels (Sá et al., 2017). In this model, both ambient and mode-specific in-vehicle exposure of air pollution are accounted for in the dose-response relation to health outcomes (Cepeda et al., 2017). The risks of traffic injuries are calculated by accounting for vehicle modes and distance travelled by both victims and vehicles. Previous studies have shown that the largest benefits can be reaped from the increase in physical activity (Mueller et al., 2015). For modelling scenarios in low and middle income countries, the challenges lie in the quality of data such as injury records and underreporting of short trips in travel surveys, which make uncertainty analysis important. Thus, a new method of data collection, such as using Google Street View, is being developed (Goel et al., 2018).
3.2.4 Participatory systems dynamic modelling (PsD)
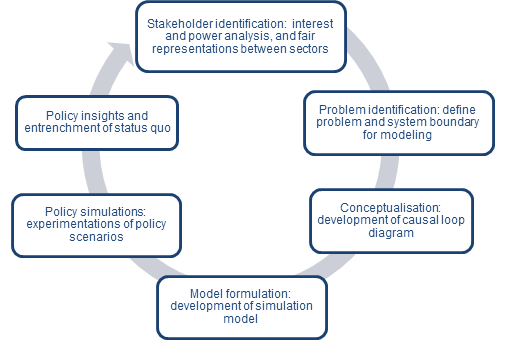
Participatory systems dynamic modelling (PsD) is a method that aims to bring changes both at the policy and the ground level through a shared learning process involving stakeholders from all relevant sectors (Macmillan et al., 2014). It facilitates understanding of the endogeneity in a complex system through feedback loops, stocks and flows process, and ensure fair representations of various sectors in public policy decision making (Eker, Zimmermann, Carnohan, & Davies, 2017). However, this process needs to take place in the early stage of policymaking; particularly at recognizing the problem to justify the inclusion of health in policy in the later stage (Macmillan et al., 2016). Figure 6 shows the general process of PsD.
4. Conclusion
In conclusion, the workshop has achieved the objectives of increasing awareness and introducing the policy assessment tools for integrating health in urban planning among the 38 international workshop participants from the Asian region. The workshop has clearly demonstrated that urban planning has great influence in determining population health, and the sustainability of cities through air quality, traffic, active living, and a population’s well being. Given the complex relationships between the environmental and health determinants in cities, the integrated health impact assessment tool, carbon calculators, and system thinking are tools that could be used to layout a clearer picture of the co-benefits of healthy urban planning with a scientific basis, and for lobbying urban planning policies that are supportive of the development of a healthy and sustainable environment for the citizens. Besides, the workshop has provided many guidelines, good practices and examples of management and implementation strategies extracted from both developed and developing countries for the reference of city planners. These examples show that the local cultures and experiences also need to be considered when incorporating health aspects in urban plans. Therefore, it is important to consult multiple stakeholders, including the local community, with a participatory approach to ensure that the programs that are carried out are sustainable to the future by themselves. In an additional note, the availability of reliable data is vital to be able to employ the assessment tools with confidence in cities, especially of developing countries where data is often lacking. These tools need to be employed early in the policymaking process to give the most significant effects. Therefore, further studies on how to utilize these tools in practice with the available data need to be explored for the planning of cities in the developing countries.
Acknowledgement
The financial support granted by the Asia-Pacific Network for Global Change (project reference CBA2018-07SY-Kwan) is duly acknowledged. The author would also like to thank the collaborating partners of the project: Prof. Dr Jamal Hisham Hashim (University Selangor), Prof. Dr Budi Haryanto (University of Indonesia), Prof. Dr Mark Stevenson (University of Melbourne), and Dr Alexandra Macmillan (University of Otago) for their support and input to the workshop.
References
- Acharya, S., Lin, V., & Dhingra, N. (2018). The role of health in achieving the sustainable development goals. Bulletin of the World Health Organization, 96(9), 591–591A. doi:http://dx.doi.org/10.2471/BLT.18.221432
- Badland, H., Whitzman, C., Lowe, M., Davern, M., Aye, L., Butterworth, I., … Giles-Corti, B. (2014). Urban liveability: Emerging lessons from Australia for exploring the potential for indicators to measure the social determinants of health. Social Science & Medicine, 111, 64–73. doi:10.1016/j.socscimed.2014.04.003
- Bartolomei, L., Corkery, L., Judd, B., & Thompson, S. (2003). A bountiful harvest: Community gardens and neighbourhood renewal in Waterloo. NSW Department of Housing and The University of New South Wales.
- Bennett, J. E., Stevens, G. A., Mathers, C. D., Bonita, R., Rehm, J., Kruk, M. E., … & Ezzati, M. (2018). NCD Countdown 2030: worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. The Lancet, 392(10152), 1072-1088. doi:10.1016/S0140-6736(18)31992-5
- Cepeda, M., Schoufour, J., Freak-Poli, R., Koolhaas, C. M., Dhana, K., Bramer, W. M., & Franco, O. H. (2017). Levels of ambient air pollution according to mode of transport: a systematic review. The Lancet Public Health, 2(1), e23-e34. doi:10.1016/S2468-2667(16)30021-4
- Chan, R. C. K., & Li, L. (2016). Entrepreneurial city and the restructuring of urban space in Shanghai Expo. Urban Geography, 38(5), 666–686. doi:10.1080/02723638.2016.1139909
- Community and Public Health. (2019). Integrated planning guide for a healthy, sustainable and resilient future: Version 3. Canterbury District Health Board, Christchurch, New Zealand. Retrieved from https://www.cph.co.nz/wp-content/uploads/IntegratedPlanningGuideV3.pdf
- Covatta, A. (2017). Density and Intimacy in Public Space: A case study of Jimbocho, Tokyo’s book town. Journal of Urban Design and Mental Health, 3. Retrieved from https://www.urbandesignmentalhealth.com/journal-3—jimbocho.html
- Creutzig, F., Baiocchi, G., Bierkandt, R., Pichler, P.-P., & Seto, K. C. (2015). Global typology of urban energy use and potentials for an urbanization mitigation wedge. Proceedings of the National Academy of Sciences, 112(20), 6283–6288. doi:10.1073/pnas.1315545112
- de Leeuw, E., & Simos, J. (Eds.). (2017). Healthy cities: the theory, policy, and practice of value-based urban planning. Springer.
- Department of Environment Malaysia. (2012). Guidance document on health impact assessment (HIA) in environmental impact assessment (EIA).
- Driscoll, R., Stettler, M. E. J., Molden, N., Oxley, T., & ApSimon, H. M. (2018). Real world CO2 and NOx emissions from 149 Euro 5 and 6 diesel, gasoline and hybrid passenger cars. Science of The Total Environment, 621, 282–290. doi:10.1016/j.scitotenv.2017.11.271
- Eker, S., Zimmermann, N., Carnohan, S., & Davies, M. (2017). Participatory system dynamics modelling for housing, energy and wellbeing interactions. Building Research & Information, 46(7), 738–754. doi:10.1080/09613218.2017.1362919
- enHealth. (2001). Health impact assessment guidelines. Commonwealth Department of Health and Aged Care, Canberra. Retrieved from http://hiaconnect.edu.au/old/files/enhealth_hia_guidelines.pdf
- Frieden, T. R. (2010). A framework for public health action: The health impact pyramid. American Journal of Public Health, 100(4), 590–595. doi:10.2105/ajph.2009.185652
- Frieden, T. R. (2004). Take care New York: A focused health policy. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 81(3), 314–316. doi:10.1093/jurban/jth118
- Goel, R., Garcia, L. M. T., Goodman, A., Johnson, R., Aldred, R., Murugesan, M., … Woodcock, J. (2018). Estimating city-level travel patterns using street imagery: A case study of using Google Street View in Britain. PLOS ONE, 13(5), e0196521. doi:10.1371/journal.pone.0196521
- Hutton, C., Nicholls, R., Lázár, A., Chapman, A., Schaafsma, M., & Salehin, M. (2018). Potential trade-offs between the Sustainable Development Goals in coastal Bangladesh. Sustainability, 10(4), 1108. doi:10.3390/su10041108
- Intergovernmental Panel on Climate Change (IPCC). (2014). Summary for Policymakers. In Edenhofer, O., Pichs-Madruga, R., Sokona, Y., Farahani, E., Kadner, S., Seyboth, K., Adler, A., Baum, I., Brunner, S., Eickemeier, P., Kriemann, B., Savolainen, J., Schlömer, S., von Stechow, C., Zwickel, T. and Minx, J.C. (Eds.), Climate Change 2014: Mitigation of climate change. Contribution of Working Group III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge University Press, Cambridge, United Kingdom and New York, NY, USA.
- Intergovernmental Panel on Climate Change (IPCC). (2001). Summary for Policymakers. In Metz, B., Davidson, O., Swart, R., and Pan, J. (Eds.), Climate Change 2001: Mitigation. Contribution of Working Group III to the Third Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge: Cambridge University Press, Cambridge, United Kingdom and New York, NY, USA.
- Levy, J. M. (2017). Contemporary urban planning. Taylor & Francis. Routledge, New York.
- Lock, K. (2000). Health impact assessment. British Medical Journal, 320(7246), 1395–1398. doi:10.1136/bmj.320.7246.1395
- Macmillan, A., Connor, J., Witten, K., Kearns, R., Rees, D., & Woodward, A. (2014). The Societal Costs and Benefits of Commuter Bicycling: Simulating the effects of specific policies using system dynamics modeling. Environmental Health Perspectives, 122(4), 335–344. doi:10.1289/ehp.1307250
- Macmillan, A., Davies, M., Shrubsole, C., Luxford, N., May, N., Chiu, L. F., … Chalabi, Z. (2016). Integrated decision-making about housing, energy and wellbeing: A qualitative system dynamics model. Environmental Health, 15(S1). doi:10.1186/s12940-016-0098-z
- Martinez, R., Lloyd-Sherlock, P., Soliz, P., Ebrahim, S., Vega, E., Ordunez, P., & McKee, M. (2020). Trends in premature avertable mortality from non-communicable diseases for 195 countries and territories, 1990–2017: A population-based study. The Lancet Global Health, 8(4), e511-e523. doi:10.1016/S2214-109X(20)30035-8
- Mueller, N., Rojas-Rueda, D., Cole-Hunter, T., de Nazelle, A., Dons, E., Gerike, R., … Nieuwenhuijsen, M. (2015). Health impact assessment of active transportation: A systematic review. Preventive Medicine, 76, 103–114. doi:10.1016/j.ypmed.2015.04.010
- Mueller, N., Rojas-Rueda, D., Basagaña, X., Cirach, M., Cole-Hunter, T., Dadvand, P., … Nieuwenhuijsen, M. (2017). Urban and transport planning related exposures and mortality: A health impact assessment for cities. Environmental Health Perspectives, 125(1), 89–96. doi:10.1289/ehp220
- Pasir Gudang chemical spill: 6 things you need to know. (14 March 2019). The Straits Times. Retrieved from https://www.straitstimes.com/asia/se-asia/johor-toxic-chemical-dumping-6-things-you-need-to-know
- Penrith City Council. (2015). Cooling the city strategy. Retrieved from https://www.penrithcity.nsw.gov.au/images/documents/waste-environment/sustainability/Cooling_The_City_Strategy.pdf
- Peters, R., Ee, N., Peters, J., Beckett, N., Booth, A., Rockwood, K., & Anstey, K. J. (2019). Common risk factors for major noncommunicable disease, a systematic overview of reviews and commentary: the implied potential for targeted risk reduction. Therapeutic Advances in Chronic Disease, 10, 204062231988039. doi:10.1177/2040622319880392
- Pineo, H., Glonti, K., Rutter, H., Zimmermann, N., Wilkinson, P., & Davies, M. (2018). Urban health indicator tools of the physical environment: A systematic review. Journal of Urban Health, 95(5), 613–646. doi:10.1007/s11524-018-0228-8
- Sá, T. H. de, Tainio, M., Goodman, A., Edwards, P., Haines, A., Gouveia, N., … Woodcock, J. (2017). Health impact modelling of different travel patterns on physical activity, air pollution and road injuries for São Paulo, Brazil. Environment International, 108, 22–31. doi:10.1016/j.envint.2017.07.009
- Stevenson, M., Thompson, J., de Sá, T. H., Ewing, R., Mohan, D., McClure, R., … & Wallace, M. (2016). Land use, transport, and population health: Estimating the health benefits of compact cities. The Lancet, 388(10062), 2925-2935. doi:10.1016/S0140-6736(16)30067-8
- Stevenson, m., & Thompson, J. (2019). Development of a prototype co-benefits calculator for low-carbon precinct design: Final report [PDF file]. Retrieved from http://www.lowcarbonlivingcrc.com.au/sites/all/files/publications_file_attachm
- Tsouros, P. E. (2008). A healthy city is an active city: a physical activity planning guide. The Regional Office for Europe of the World Health Organization, Denmark, 9.
- United Nations General Assembly. (1987). Report of the world commission on environment and development: Our common future. Oslo, Norway: United Nations General Assembly,
Development and International Co-operation: Environment. - Videira, N., Antunes, P., & Santos, R. (2017). Engaging stakeholders in environmental and sustainability decisions with participatory system dynamics modeling. In Gray, S., Paolisso, M., Jordan, R., & Gray, S., Environmental modeling with stakeholders (pp. 241-265). Springer, Cham.
- Walsham, G. (2019). Health information systems in developing countries: Some reflections on information for action. Information Technology for Development, 26(1), 194–200. doi:10.1080/02681102.2019.1586632
- Wancharoen, S. (2018). These streets were made for walkin’ — or they soon will be. Bangkok Post. Retrived at: https://www.bangkokpost.com/thailand/special-reports/1495002/these-streets-were-made-for-walkin-or-they-soon-will-be
- Webb, R., Bai, X., Smith, M. S., Costanza, R., Griggs, D., Moglia, M., … Thomson, G. (2017). Sustainable urban systems: Co-design and framing for transformation. Ambio, 47(1), 57–77. doi:10.1007/s13280-017-0934-6
- Wheeler, S.M. & Beatley, T. (Eds.). (2014). The sustainable urban development reader (Third Edition). The Routledge Urban Reader Series. New York: Routledge doi:10.4324/9781315770369
- WHO, 2014. Health in All Policies (HiAP) framework for country action. Health Promotion International, 29(suppl 1), i19–i28. doi:10.1093/heapro/dau035.
- Winkler, S. L., Anderson, J. E., Garza, L., Ruona, W. C., Vogt, R., & Wallington, T. J. (2018). Vehicle criteria pollutant (PM, NOx, CO, HCs) emissions: How low should we go? npj Climate and Atmospheric Science, 1(1). doi:10.1038/s41612-018-0037-5
- Woodcock, J., Givoni, M., & Morgan, A. S. (2013). Health impact modelling of active travel visions for England and Wales using an integrated transport and health impact modelling tool (ITHIM). PLOS ONE, 8(1), e51462. doi:10.1371/journal.pone.0051462